Cervical Spine Disc Replacement
DR PREM PILLAY
SPINE SPECIALIST,
NEUROSURGEON AND SPINE DISC REPLACEMENT EXPERT
Cervical Spine artificial disc replacement (Cervical Spine-ADR) is an advanced surgical and Microsurgical technique designed to preserve motion in the cervical spine by replacing damaged or degenerated discs with artificial ones. For the right patients it is an excellent treatment that avoids many of the problems of the older treatment of spinal fusion explains Dr Prem Pillay, a Spine Specialist who is experienced with both spinal fusion and artificial disc replacements.
Indications
Cervical Spine ADR is typically indicated for patients suffering from:
- Cervical Disc Herniation: When a disc protrudes or ruptures, causing spine nerve and/or spinal cord compression that can cause myelopathy and/or radiculopathy. Patients with myelopathy can have progressive weakness of the arms and legs.
- Cervical Radiculopathy: Pain, weakness, or numbness radiating from the neck into the arms due to spine nerve root compression.
- Cervical Degenerative Disc Disease: Progressive wear and tear of the discs leading to loss of disc height, instability, and pain.
The procedure is considered when:
- Conservative treatments like physical therapy and pain medication have failed.
- Patients exhibit symptoms such as neck pain, arm pain, numbness, or weakness.
- Imaging including X-rays, CT Spine and the better MRI of the Spine confirms disc pathology that correlates with clinical symptoms.
Materials Used
Various materials are employed in the construction of artificial cervical discs:
- Polyethylene (PE): Often used for the core or bearing surfaces due to its durability and low friction.
- Cobalt-Chrome (CoCr) Alloys: Common in endplates for their strength and biocompatibility.
- Stainless Steel: Less commonly used due to MRI incompatibility but still found in some designs.
- Titanium (Ti) Alloys: Known for their excellent biocompatibility, often used for endplates or as coatings to promote bone ingrowth.
- Polycarbonate Urethane (PCU): Used in some discs for its cushioning properties.
- Ultra-High-Molecular-Weight Polyethylene (UHMWPE): A variant of polyethylene with enhanced durability for bearing surfaces.
The choice of materials focuses on durability, biocompatibility, and their ability to mimic the natural biomechanics of the cervical spine. Most Neurosurgeons use the best ADRs that have good results and are FDA and/or CE regulated and registered.
Techniques
The surgical technique for Cervical Spine-ADR involves:
- Anterior Approach: A small incision (1-2 inches) is made on the front or side of the neck to access the cervical spine. Xrays are used for localization. High quality visualization is used with special Spine Microscopes and microinstruments.
- Disc Removal: Under the Microscope the Neurosurgeon removes the damaged disc, taking care to preserve the surrounding structures like the posterior longitudinal ligament.
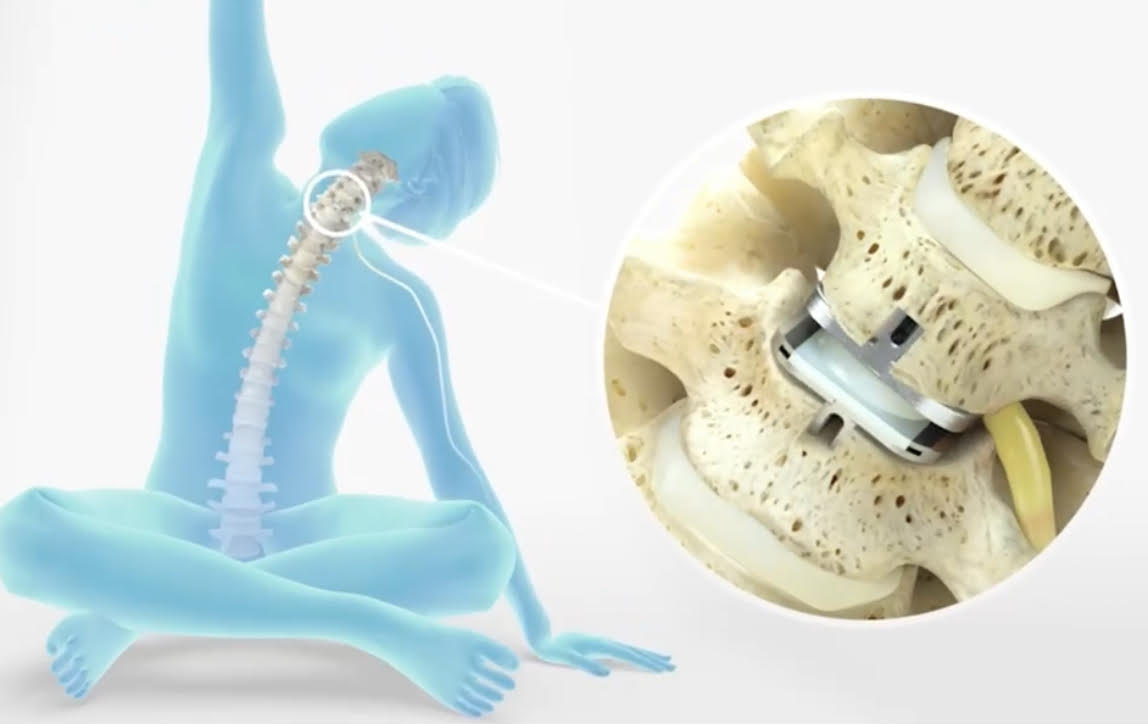
- Disc Replacement: An artificial disc is inserted into the disc space. This can be:
- Single-piece designs, where the implant is one unit with metal endplates and a polymer core.
- Two and three-piece designs, with two endplates and a mobile core, allowing for more natural motion.
- Fixation: Techniques to ensure the implant remains stable include keels, spikes, wire mesh, or specialized coatings like hydroxyapatite to promote bone ingrowth.
- Postoperative Care: Unlike fusion, patients typically do not need a cervical collar, or only use it for a short time when out of the home or office, promoting faster recovery, Most patients have a better quality of recover in a shorter time as compared with fusion.
Why Cervical Spine ADR is Better than Spinal Fusion
- Motion Preservation:**
C-ADR maintains segmental motion, which can reduce the risk of adjacent segment disease where adjacent discs degenerate faster due to increased stress.
- Faster Recovery:
Patients undergoing C-ADR can often return to work and normal activities sooner than those with spinal fusion due to the lack of bone fusion time.
- Lower Revision Rates:
Studies indicate that patients with C-ADR have lower rates of revision surgery or supplemental fixation procedures compared to ACDF.
- Improved Clinical Outcomes:
Long-term follow-up studies have shown significant improvements in neck disability index scores, pain, and overall patient satisfaction with C-ADR.
- Reduced Stress on Adjacent Segments:
By preserving motion, C-ADR puts less stress on the vertebrae above and below the surgical site, potentially reducing future degenerative changes.
- Biomechanical Advantage:
Artificial discs can mimic the natural disc’s function, allowing for more physiologic motion and potentially reducing the risk of further disc degeneration.
In conclusion, cervical artificial disc replacement offers a motion-preserving alternative to traditional spinal fusion with benefits including faster recovery, lower rates of subsequent surgeries, and potentially better long-term health outcomes for the cervical spine. The choice between ACDF (fusion) and ADR (replacement) should be made after a comprehensive evaluation by a Neurosurgeon spine specialist, considering the patient’s overall health, the specifics of their spinal condition, and their lifestyle needs.
With many years of experience in treating Cervical Herniated Discs (Slipped Discs) and access to the latest technological advancements, Dr Prem Pillay aims to offer patients the highest standard of care. From accurate diagnosis to tailored treatment plans, our approach aims to ensure the best possible outcomes for individuals affected by this challenging condition.
If you or a loved one has been diagnosed with a cervical spine problem, we encourage you to seek consultation with our specialized team. Together, we can develop a comprehensive evidence based and personlized treatment strategy that addresses your unique needs and provides the best chance for a positive outcome.











